

The Body’s Quiet Signals
What Your Nails, Tongue, and Skin Reveal Before Any Labs Are Drawn


Long before any visit to a physician or any labs are drawn, your body has already been talking. Most people have just never learned the language.
A patient came to me last month with a large binder filled with pages upon pages of reports. Three years of work-ups, four practitioners, sixteen specialty panels. Everything came back, in her words, “annoyingly normal.” She handed me the binder, sat down, and said, “I’ve been told I’m fine more times than I can count. I don’t feel fine.”
I didn’t open the binder.
I asked her to stick out her tongue. Then I asked to see her hands.
In the first ninety seconds before a lab value was reviewed her body had already told me where to look. The binder, when I finally opened it, only confirmed it.
This post is about that ninety seconds.
Why visible signs matter
For all of medical history physical signs and symptoms were not something to be ignored rather a window into your body’s health. Physicians developed the keen clinical skill of recognizing disease states based on clinical presentation.
Sadly most of medicine now reduces you to numbers on a piece of paper, and then it dismisses you when they are “in range”. What gets lost in that process is the part of your physiology that doesn’t need a lab to be measured. The part that’s literally hanging off the ends of your fingers, sitting in your mouth, and looking back at you in the mirror every morning.
Your skin, your nails, your tongue and your eyes give you constant insight into the metabolic, immune and nervous system processes occurring in your body. They externalize what the inside of your body can’t fully resolve. Long before a marker on a comprehensive metabolic panel drifts into “abnormal,” your body has already been running a public broadcast about what’s actually happening underneath.
None of these signs are diagnostic on their own. That isn’t the point. The point is orientation. When someone has been told for the third time that “everything looks fine,” a visible sign is often the first thing that says: no, look here next.
The Tongue
Your tongue regenerates roughly every two weeks. Whatever you see in the mirror today is, in effect, a fourteen-day report card on inflammation, hydration, B-vitamin status, and your gut terrain.
A few patterns worth knowing:
Scalloped edges (teeth marks along the sides). The tongue is swollen against the teeth. Often points to fluid imbalance, B-vitamin depletion, or the kind of “spleen qi” pattern that, in chinese medicine terms, tracks with poor nutrient absorption and chronic gut inflammation.
A thick white coating that won’t brush off. Frequently a candida or biofilm signal. The mouth is the front porch of the gut, and what you see on the tongue often mirrors what’s living in the rest of the digestive tract.
Cracks down the center. Long-standing inflammation, often digestive in origin. The deeper and more persistent the crack, the longer the pattern has been present.
A pale tongue. Iron, B12, or protein insufficiency. Pair this with brittle nails and you have one of the most common silent depletion patterns I see in patients with chronic illness.
A red, smooth, glossy tongue. Often reflects the significant deficiencies of some major nutrients including riboflavin, niacin, pyridoxine, vitamin B12, folic acid, iron, zinc, and vitamin E. It can also mean, protein-calorie malnutrition, candidiasis, Helicobacter pylori colonization, and diabetes mellitus. This can also be an important sign of developing autoimmune conditions as Chiang et al found the serum gastric parietal cell antibody (GPCA), thyroglobulin antibody (TGA), and thyroid microsomal antibody (TMA) positivities in 26.7%, 28.4%, and 29.8% of patients with this type of tongue presentation.1
Look at your tongue in the mirror tomorrow morning, before you’ve eaten or brushed. That’s the truest read.
The Nails

Your fingernails grow about 3 millimeters a month. That means a full nail represents roughly six months of metabolic history written in keratin. If you know what to look for, you can read it.
Beau’s lines. Horizontal ridges that run across the nail bed. Each one marks a moment when your body diverted resources away from non-essential tissue building — a high fever, a major stressor, a surgery, a viral reactivation, a strep infection, sometimes an emotional event severe enough to register physiologically. These can also be a sign of something deeper that is interfering with the blood flow to your nail matrix with the most common being Diabetes, Hypothyroidism and Peripheral artery disease (PAD). Patients are often surprised to learn you can roughly date these. Multiply the distance from the cuticle by the growth rate, and a Beau’s line becomes a timestamp.
Spoon nails (koilonychia). Nails that curve up at the edges instead of out. Iron deficiency is the classical cause, but in autoimmune patients it often signals chronic inflammation blocking iron utilization rather than true dietary deficiency. The lab signature for this is high ferritin with low iron saturation as it is inflammation hoarding iron rather than the body lacking it.
White spots (leukonychia). Often blamed on minor trauma, and sometimes that’s accurate. But persistent or recurring white spots track with zinc depletion, and zinc is one of the most consistently low minerals I see in chronic immune dysregulation. This is because chronic cadmium burden, parasites, and other chronic infections all utilize zinc at a faster rate than we replace it.
Longitudinal ridges running cuticle to tip. A normal feature of aging in some cases — but when they appear early, deeply, or alongside brittleness, they often track with B12, biotin, or connective tissue cofactor depletion. Many times this is often also a sign of Hypothyroidism and showcases that your metabolism has slowed down causing dry, brittle, and ridged nails. Liver disease, chronic kidney disease and low oxygen states can also cause these vertical ridges.
Brittle, peeling, splitting nails. This is often blamed on iron, selenium, protein, or zinc deficiencies (which can be true) but the upstream question is always why. As I have written elsewhere: deficiencies are rarely just about what you eat. They can be driven by toxins, infections, or parasites interfering with absorption, storage, or utilization. Additionally in the case of brittle nails heavy metals like mercury, arsenic and lead interfere with keratin (a sulfur-rich protein) cross-linking and mineral balance in the nailbed2, fungal infections like Onychomycosis alter biotin metabolism and bacterial infections like Borrelia disrupt collagen production above and beyond altering digestion and absorption of nutrients.
The nail is the slowest-turning of the visible tissues, which makes it the most honest. By simply looking at the nails we can begin to orient ourselves the possibilities of what processes are going on beneath the surface.
The Skin
The skin is your largest immunological organ. It is also the most visible. What shows up there is rarely cosmetic it’s the outward expression of your inner terrain. Instead of seeking to hide, conceal or obfuscate skin imperfections we should be seeking to understand why they are there to resolve them from the inside out.
Keratosis pilaris (the rough, fine bumps on the backs of the upper arms and thighs). Often misread as a skin issue. It’s actually a strong indicator of essential fatty acid status, vitamin A metabolism, and oftentimes gut barrier function. Patients with chronic gut inflammation absorb fat-soluble vitamins poorly, and keratosis pilaris is one of the first places that shows.
Perioral dermatitis (the rash around the mouth, sometimes the nose). I’ve come to read this as a methylation, gut microbiome, and topical-product story converging at once. It rarely resolves with steroid creams, and when it does, it usually returns. Address the upstream pattern and it tends to clear.
Bartonella-pattern striae. Faint linear marks, often pinkish or purplish, that look like stretch marks but appear in places stretch marks shouldn’t (the sides of the torso, the flanks, the inside of the upper arms). In the right clinical context, they raise the question of vascular pathogens — Bartonella in particular. This particular issue is imperative to understand as I have seen many young, otherwise healthy people berate themselves for having “stretch marks” when in fact it is the outward manifestation of an undiagnosed Bartonella infection.
Persistent itch, prickling, or “things crawling under the skin” sensations without an obvious dermatological cause. I list this last on purpose. It deserves to be taken seriously, not pathologized as anxiety. It can track with toxic burden, mast cell activation, or stealth infections. Patients who report this and get dismissed have been telling the truth all along.
The Eyes
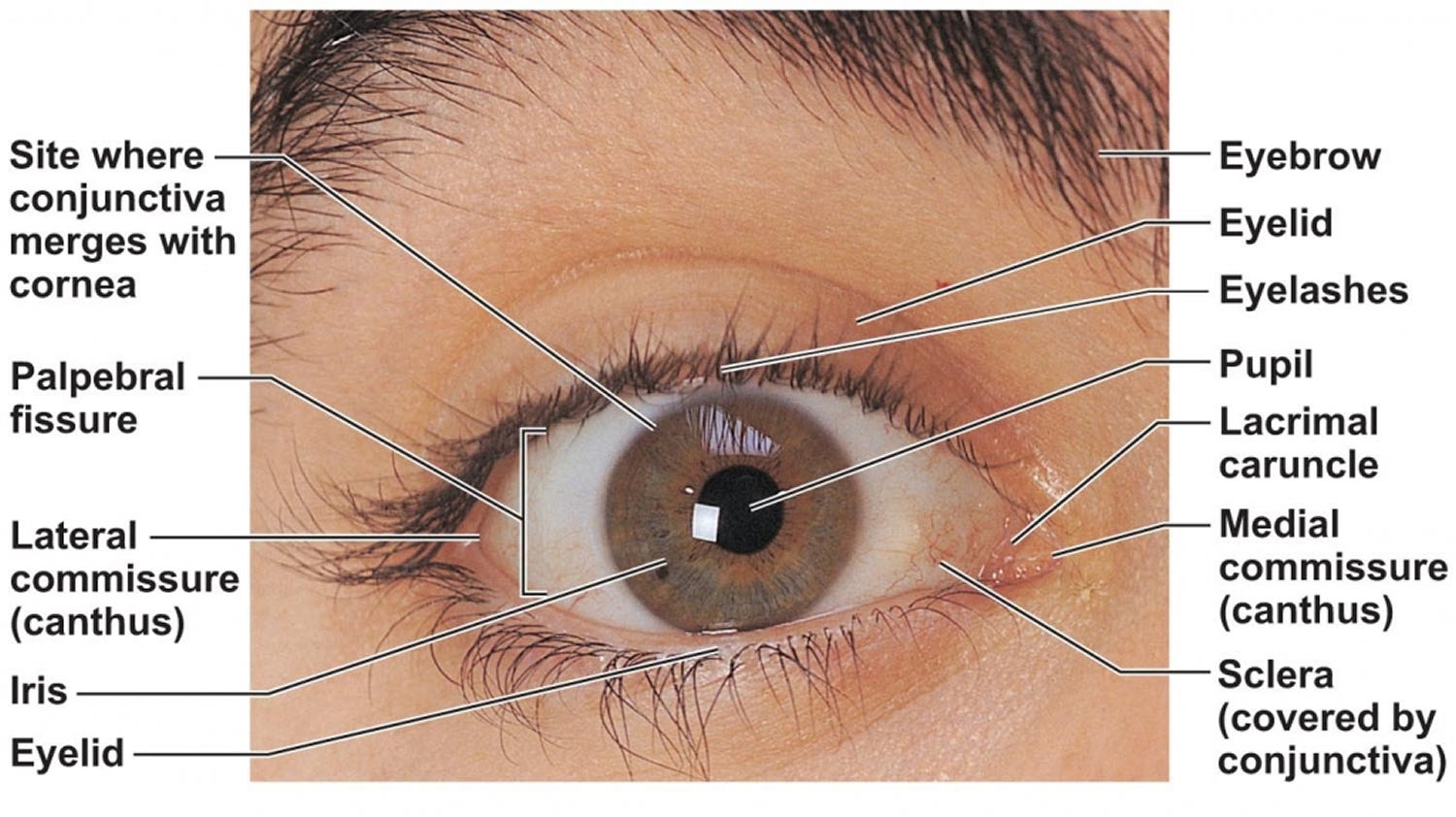
The eyes are the window to the soul and to the body but often get the least amount of attention in standard medicine. Being able to observe patterns in the eyes gives us reliable orientation on what to look at more deeply.
Sclera color. The white of the eye should be white. A faint yellow tint (even a tint) points to liver clearance under stress before bilirubin ever rises out of “normal” on a panel. A blue-grey sclera points to iron deficiency anemia and connective tissue disorders that requires deeper investigation.
Arcus (a pale ring around the iris). In someone over sixty, often unremarkable. In someone under fifty, it’s worth noting as it tracks with cholesterol metabolism and sometimes oxidative stress patterns that are easy to confirm on a particle-size lipid panel.
Foamy white/gray patches on conjunctiva (Bitot spots). Points to a vitamin A deficiency on the surface and deeper it orients to a fat malabsorption problem with underlying bile/pancreatic issues3.
Brown/green ring at corneal edge (Kayser–Fleischer ring). Classically thought of only is Wilson’s disease this sign points to copper accumulation within the body and often more importantly for most people it suggests a liver condition where the flow of bile has been slowed as a results of chronic toxin burden and often points to poor detoxification and gut health issues.
Conjunctival redness or persistent dryness. Often dismissed as allergies. Frequently the first visible expression of Sjögren’s-pattern dysregulation, sometimes years before antibodies turn positive on a lab.
What this is and what it isn’t
Read your tongue, your nails, your skin, your eyes. Notice what you see. Compare what you see to what you read above.
But understand: none of this is diagnostic in and of itself. A scalloped tongue alone does not give you a diagnosis. White spots on your nails alone do not tell you your zinc is low. A patch of keratosis pilaris does not confirm vitamin A insufficiency.
What these signs do is orient. They give you a starting place when the labs all came back “normal” and you were sent home with nothing but a shrug. They tell you where to look next. They tell a clinician who actually listens what to investigate further, what to test, what to rule out, and what to take seriously when the conventional system has stopped taking you seriously.
The body has never not been talking to you. The work is learning to listen in the language it’s actually using.
If your labs say normal but your body says otherwise
The gap between what the standard panel shows and what your body keeps telling you is exactly the conversation worth having. It’s not in your head. It’s in your tongue, your nails, your skin, your eyes, and probably in a half-dozen markers nobody thought to test for.
If you’d like to talk about what’s actually going on in your case, you can book a free 15-minute health strategy call here. My team will hear you out, ask the right questions, and tell you honestly whether we’re the right fit to help you map what’s actually happening.
Your body isn’t broken. It’s been telling you the truth all along.
Until next time,
P.S. On Saturday, May 16, I’m doing a live walkthrough of real labs for paid subscribers — the foundational twelve labs every autoimmune patient should run first, and what to do when the standard panel says you’re fine. If that sounds useful, the paid subscription gets you in.
Chiang CP, Chang JYF, Wang YP, Wu YC, Wu YH, Sun A. Significantly higher frequencies of anemia, hematinic deficiencies, hyperhomocysteinemia, and serum gastric parietal cell antibody positivity in atrophic glossitis patients. J Formos Med Assoc 2018;117:1065e71.
Lotah HNA, Agarwal AK, Khanam R. Heavy metals in hair and nails as markers of occupational hazard among welders working in United Arab Emirates. Toxicol Res. 2021 Feb 17;38(1):63-68.
Gilbert C. The eye signs of vitamin A deficiency. Community Eye Health. 2013;26(84):66-7.